Dr. Eugene Fine and I will described the problem as laid out in our campaign at Experiment.com. The campaign intends to follow-up Dr. Fine’s pilot study of ten advanced cancer patients on ketogenic diets and the in vitro projects that we are carrying out in parallel.We got good feedback and some good questions and we want to continue the scientific interaction and keep the community intact that was started on the “lab notes” at Experiment. We will recapitulate some of the points made during the campaign and you can “ask the researchers” in comments.
“What makes you think ketone bodies will help?”
We and others have carried out experiments that show the effects of ketone bodies on cancer cells in culture, as diet for patients with advanced cancer or as adjuncts to other modalities. Most direct experimental studies, however, must be considered preliminary and it is reasonable to ask why we thought ketone bodies might help.
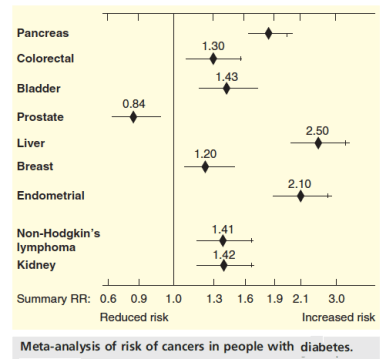
The evidence supporting carbohydrate restriction, or specifically ketogenic diets in cancer remains largely indirect and speculative. Our recent perspective summarized some of the relevant evolutionary and mechanistic factors: the central theme rests with the role of the glucose-insulin axis in promoting growth and proliferation, the predominant characteristic of cancer sells. So it has been observed for some time that patients with diabetes have higher risk of cancer. Epidemiological and other kinds of studies are generally consistent with the idea although different cancers are more or less closely associated with diabetes. Drugs employed as diabetes therapy, particularly metformin, have been found to have beneficial effects in cancer as well. Metformin reduces the risk of developing cancer although the effects on mortality are not clear cut. We made the case, in our critical review that dietary carbohydrate restriction is the first line of treatment for type 2 diabetes and the best adjunct for pharmacology in type 1 diabetes.
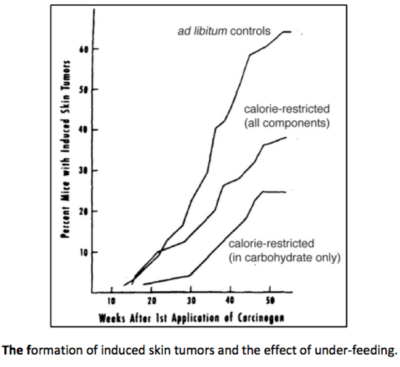
The association between cancer and diabetes in combination with the benefits of carbohydrate restriction in diabetes constitute one big connection. In dietary approaches, however, it is total caloric reduction that has received the most attention and, in fact, experiments show that if implemented as stated, calorie restriction represents a reliable approach to prevention and treatment of cancer, particularly in animal models. It is unknown how much of the effect is due to de facto reduction in particular macronutrients but when tested, carbohydrate reduction as the means of reducing calories prove most effective. We cited an important study by Tannenbaum. He found, in 1945 (!) that a carcinogen-induced sarcoma in mice was repressed by reduction in total calories but if reduced by specifically lowering the carbohydrate intake, there was an enhanced response.
Impressive cancer prevention with calorie restriction in animal models has been repeated many times. Oddly, the protocol is most often presented as caloric restriction. Odd in that this appears in sophisticated scientific papers where the downstream effects of the stimulation may pinpoint twenty molecular components and where the molecular targets of the “nutrients” are characterized and may specifically be the insulin receptor and the related IGF-1 (insulin-like growth factor -1) receptor. (Insulin is probably most important in that it stimulates IGF-1 activity by reducing the levels of the associated binding proteins). In these studies, where total caloric reduction is the independent variable, the involvement of insulin and the insulin-dependent downstream pathways have been shown to be involved.
It is now appreciated that the Warburg effect, the apparent reliance of tumors on glucose for fuel, is a key observation that has been insufficiently explored. The effect provides motivation and clues for exploring the metabolic approach to cancer. Warburg thought that all cancers showed this phenotype which is not true but a large number do; of significance is that one that does not, prostate cancer, is the outlier in the figure above on relation to diabetes. The next post will start from some basic biochemistry and explain why (and how) we think that the Warburg effect points to the potential value of ketogenic diets.

